Introduction: Near-total Intestinal Aganglionosis (N-tIA) extending into high jejunum results in a severe short bowel state with large jejunostomy losses, and increased mortality from TPN/sepsis liver injury and loss of venous access, and life-long TPN dependence for those with <20cm jejunum. The alternatives are Autologous Gastrointestinal Reconstruction (AGIR) or Bowel Transplant. We present a female child who underwent Bowel Expansion, Sequential Autologous Bowel Lengthening with SILT (Spiral Intestinal Lengthening) followed by LILT (Longitudinal Intestinal Tailoring and Lengthening), and the addition of a prejejunostomy patch of aganglionic right colon, with an ongoing and improving outcome.
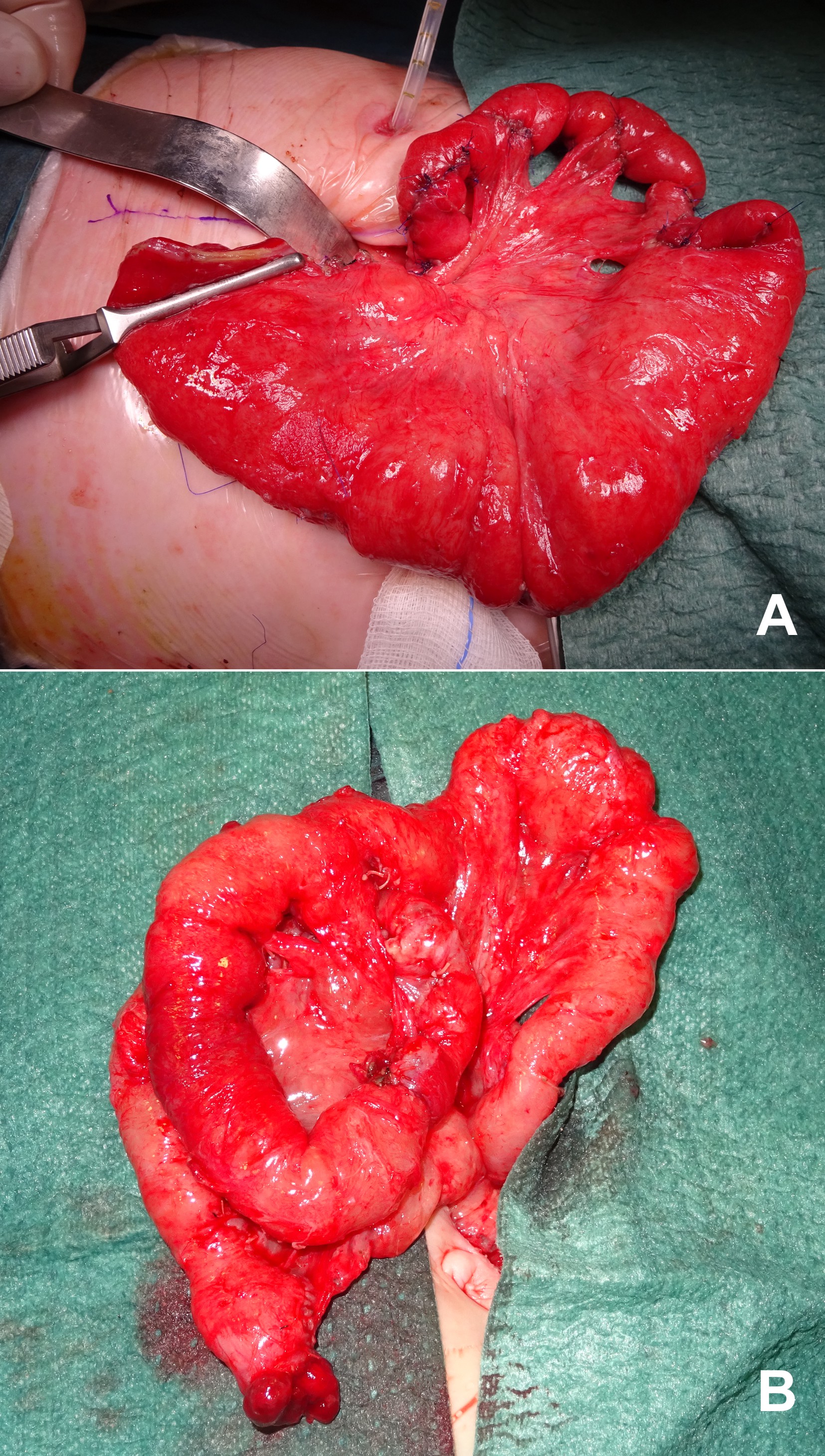
Methods: A 14-day old female child with N-tIA and 20cm of ganglionic residual jejunum from the ligament of Trietz, was initially treated by jejunostomy at 50cm from Treitz, retaining 30cm of aganglionic jejunum. At 15months the aganglionic jejunum was excised and the dilated proximal ganglionic 20cm were lengthened by SILT to a total of 50cm (fig1A). The stoma was closed around a 16F Pezzer catheter that was brought out onto the abdominal wall as a Tube Jejunostomy. Timed catheter clamping over 5 months induced Controlled Bowel Expansion, and was followed by LILT (fig1B) to an increased total jejunal length of 80cm.
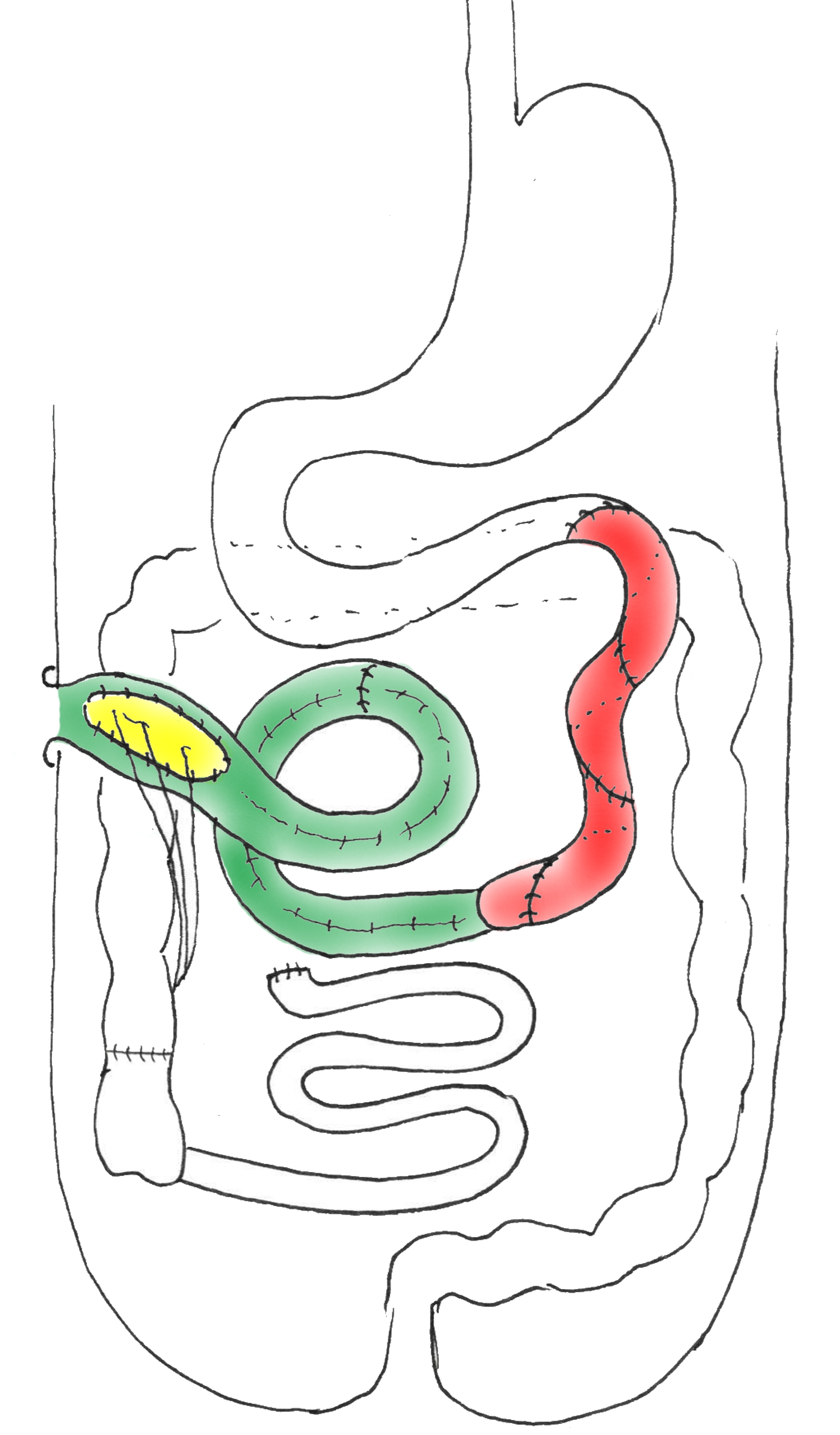
At 29months of age 10cm of opened ascending colon was patched to the side of the distalmost jejunum just proximal to a permanent jejunostomy stoma (fig2).
Results: At 5years of age total TPN caloric requirement has decreased from 100% to 55%, and her Body Mass Index is 15.4 at the 50th centile for her age. Neurological function is normal for her age. Largely after the colonic patch her stoma output reduced from 130ml/kg to 30ml/kg.
Conclusion: Patients with N-tIA with a residual short bowel state benefit from AGIR designed to increase full thickness bowel volume and enhancing intestinal adaptation. Following controlled bowel expansion, sequential lengthening by SILT and LILT, and an ascending colon patch (endogenous GLP2?) our patient has had a 50% reduction in TPN requirement and has shown sustained physical and mental growth and an improved quality of life. We recommend management spanning several years by Sequential Autologous Gastrointestinal Reconstruction (expansion, lengthening, increased mucosal contact techniques) to enhance intestinal adaptation and absorption, and with no cut-off point for referral for Intestinal Transplantation.
.jpg )