Background: Donor/Recipient CMV mismatch is a controversial exclusion criteria for graft selection in intestinal transplantation. Case experience was reviewed to determine impact of D/R CMV serostatus on patient and graft survival, CMV disease and resistance.
Aim: To determine the impact of D/R CMV serostatus on patient and graft survival and CMV disease in recent era.
Methods: All children with primary Intestinal transplant between 2001-2016 were analyzed for CMV D/R serostatus and patient outcomes.
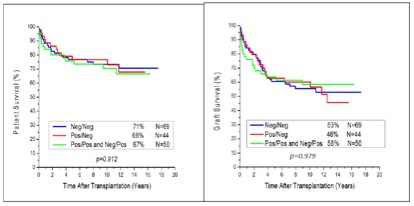
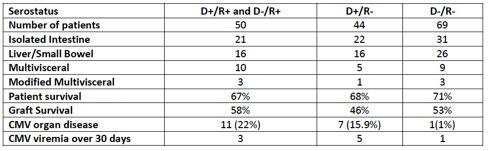
Results: 163 Children received primary allografts (74 isolated intestine, 58 liver intestine, 24 multivisceral, 7 modified multivisceral grafts) between 2001-2016. Patient and graft survival were 69% and 53% at 109 months. Outcomes by CMV serostatus are listed in Table 1. CMV prophylaxis consisted of ganciclovir X 14 days in all cases except CMV +/- where the ganciclovir course is followed by 3 months of PO valganciclovir and CMV immunoglobulin at 72 hours, 2,4,6,8, 12, and 16 weeks post operatively.
Conclusions
- CMV serostatus for D/R is an important consideration in intestine transplantation but mismatch is not associated with increased graft or patient morbidity.
- Tissue-invasive CMV disease is significantly more frequent in recipients that receive organs from CMV + donors but can be managed with monitoring and current treatment.
.jpg )