Introduction: Ex vivo surgery – explant organs en bloc, resect and reconstruct outside of the body in the cold preservation, and reimplant unaffected parts of organs - may improve a chance at complete (R0) resection for conventionally unresectable tumors. For the tumors involving superior mesenteric vasculature, patients typically present with persistent abdominal pain and sometimes intestinal/biliary obstruction, intestine-tumor fistula, or chylous ascites. Attempting to resect such tumors in vivo may not only result in incomplete tumor resection, but also loss of bowel integrity by vascular compromise and subsequent organ ischemia. Here we describe our experience of ex vivo approach for effective tumor resection with intention of maximum bowel preservation.
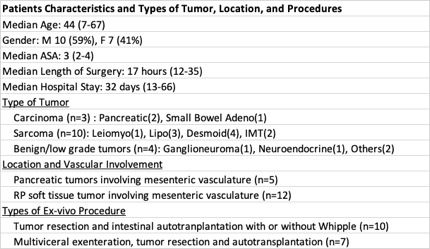
Methods: We retrospectively reviewed 17 consecutive patients who underwent ex vivo surgery and intestinal autotransplantation at our institution 2009-2018.
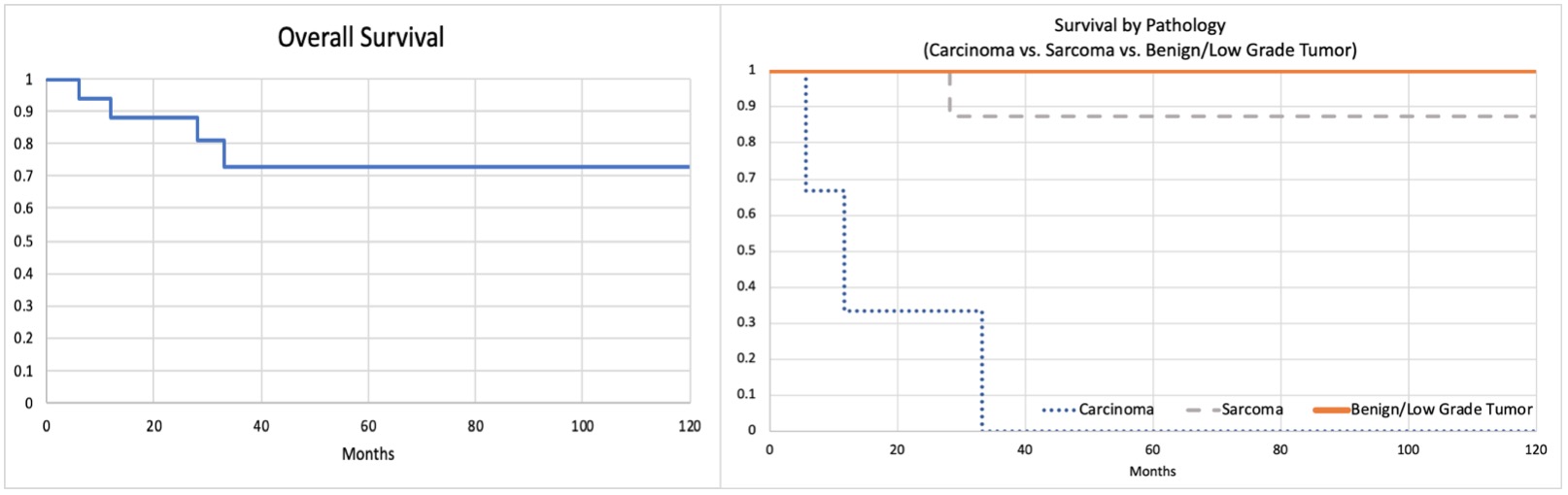
Results: Ex vivo surgery was performed for patients with a tumor involving mesenteric vasculature from pancreatic origin (n=5) or retroperitoneal soft tissue tumor (n=12). The procedure was chosen based on tumor location and degree of vascular involvement, which resulted tumor resection with intestinal autotransplantation with/without Whipple procedure (n=10) or multiviceral exenteration and autotransplantation (n=7). Of these seventeen patients, two patients had inadequate perfusion of intestine autograft which was explanted at planned second look laparotomy, requiring TPN and intestine transplantation. For fifteen patients with successful intestinal autotransplantation, average remaining bowel length was 320cm with minimum length being 190cm with IC valve. For GI complications, two patients had prolonged ileus of which one patient required temporary TPN support. Two patients had prolonged high output ileostomy and one patient had chronic diarrhea. Tumor types were carcinoma (n=3), sarcoma (n=10), or benign/low grade tumors (n=4). The overall survival was 88%/73%, at 1-year/5-year, respectively. Perioperative (90-day) mortality was 0%. 88% (15/17) patients had R0 resection, and 65% (11/17) had no recurrence to date with median follow-up of 2 years.
Conclusions: With experience, in selected patients with conventionally unresectable tumors involving superior mesenteric vasculature, ex vivo tumor resection and intestinal autotransplantation can offer effective tumor removal with a reasonable bowel preservation.
.jpg )