Multivisceral transplant (MVT) for ESLD and stage IV portomesenteric vein thrombosis (PVT), is a highly complex procedure fraught with life-threatening thrombo-hemorrhagic complications. Preoperative visceral arterial embolization is a means to facilitate exenteration and minimize bleeding.1 Technical success, however, has to be measured clinically through the attainment of poorly perfused/ischemic viscera, and may be further validated by pathological exam of the eviscerated organs.
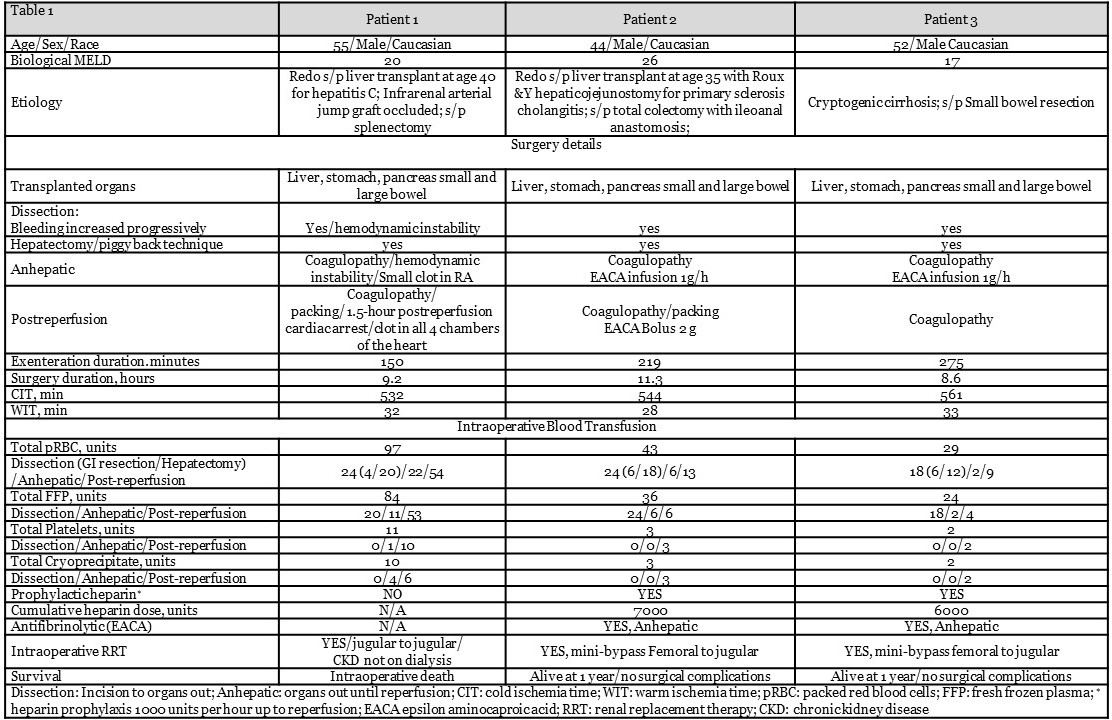
We present 3 such patients, (2 were redo), who underwent visceral arterial embolization prior to MVT. A descriptive analysis of recipients is presented in Table 1.
A comparative analysis of the embolization procedure, visceral organs perfusion during exenteration, and gross pathological examination of the visceral specimen is outlined in Table 2.
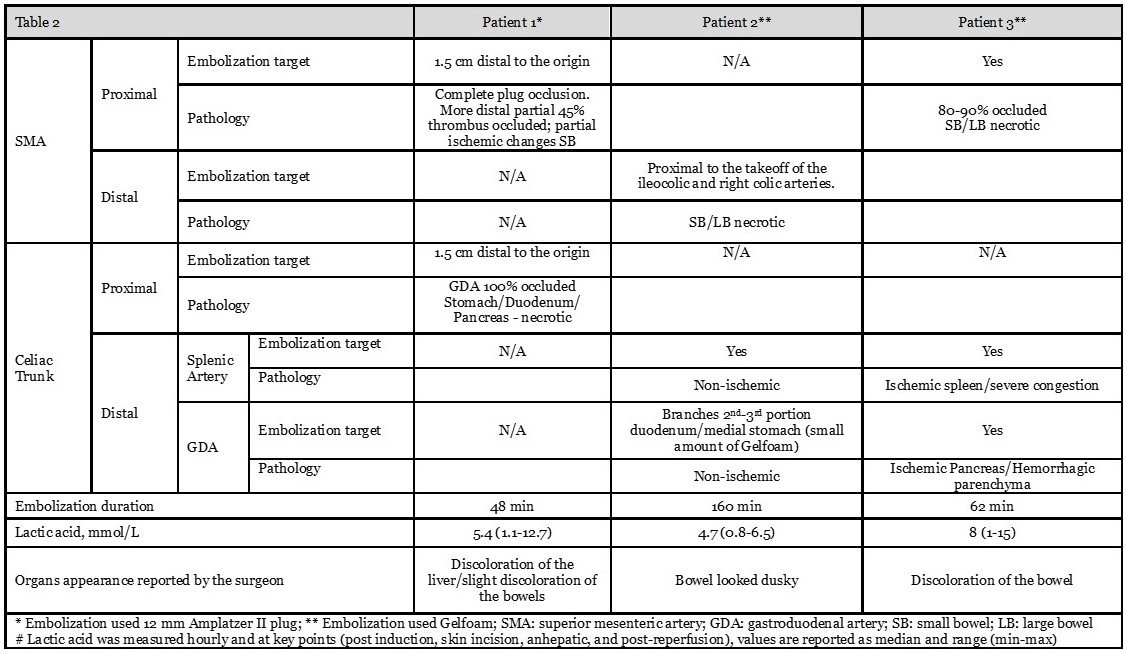
Patient #1 had an angiographically confirmed initial successful deployment of a proximal celiac trunk plug, but in the laparotomy liver perfusion was preserved. Pathological exam of eviscerated organs confirmed the dislodgement and distal migration of the plug into the GDA. In order to preserve liver flow, patients #2 & 3 underwent selective embolization of the splenic and gastroduodenal branches of the celiac trunk. Successful embolization of the SMA was achieved in all 3 patients, and facilitated resection of ischemic intestine, pancreas and spleen with reduced blood loss (4/6/6 pRBCs). However, in all 3 cases a severe coagulopathy with significant hemorrhage occurred during hepatectomy (20/18/12 pRBCs). Patient 1 suffered a full blown DIC, intravascular thrombosis and severe hemodynamic instability that led to intraoperative death. Coagulopathy in patient 2 and 3 subsided post-reperfusion. Circulatory exclusion of the liver in MVT is frequently associated with the development of life-threatening coagulopathy. Heparin prophylaxis is warranted to control consumptive coagulopathy and minimize risk of intravascular thrombosis. Effective heparinization allows a safer management of hyperfibrinolysis with antifibrinolytics when indicated.2
In conclusion, MVT in recipients with “hostile abdomen” is associated with severe hemodynamic, hemorrhagic, and hemostatic perturbations. Hepatic sparing embolization of gastrointestinal viscera facilities exenteration and effectively reduces blood loss. Coagulopathy, however, remains a life-threatening thrombo-hemorrhagic risk, and heparin prophylaxis with diligent hemostatic management are indicated.
.jpg )