Introduction: Short bowel syndrome (SBS) remains the main cause of Intestinal Failure (IF). The management at a comprehensive unit assures an adequate evaluation, maximizing opportunities to achieve intestinal autonomy.
We aim to report the long term results of medical and surgical rehabilitation of patients (pts) with type III IF (III-IF) and to develop a formula to predict PN independency based on anatomical and clinical variables.
Material and Methods: Retrospective analysis of a prospective database of III-IF adult pts, that underwent Autologous Gastrointestinal Reconstruction Surgery (AGIRS) from 3/2006 to 08/2018. Age, gender, primary diagnosis, pre-surgical anatomy, post-surgical intestinal length (PSIL): grouped as a , b and c (table 1); post-surgical anatomy; (PSAT) type: 1, 2 or 3; presence of ICV, PN reduction >2/7 days. Statistical analysis was done on SPSS v2.
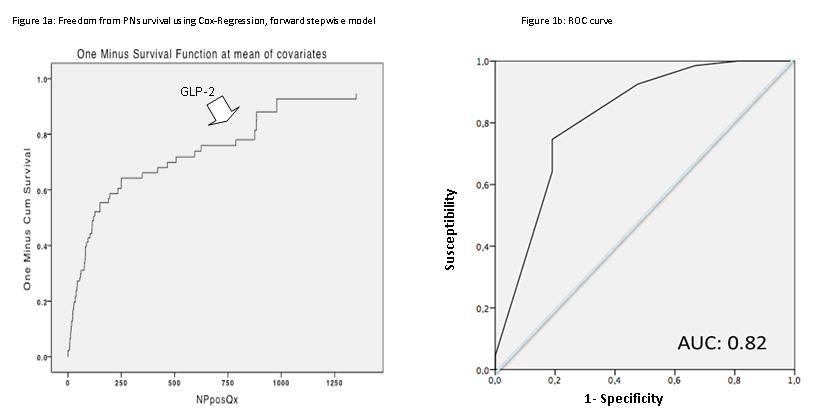
Results: From 259 adults pts with IF, 185 (71%) had III-IF. AGIRS was performed in 88 pts; mean age: 49.5 ± 14.6 years; 51 female. Primary diagnosis: post op IF 48, ischemia 20, post bariatric surgery 5, others 15. The anatomy at first visit was: type 1 in 78 , type 2 in 3, and type 3 in 7 pts. Mean time on PN before AGIRS was 313.14 ± 483.8 days. PSAT was type 1 in 3, type 2 in 26 and type 3 in 59 pts. The mean PSIL was 159 ± 103.4 cm; according to the PSIL, 13 pts were type a; 16 type b and 59 type c.:. Mean Time on PN after AGIRS was: 817.6 ± 661.3 days. Table 1 shows outcomes based on PSIL and PSAT. Eight pts were started on teduglutide (TED); the mean time on therapy is 764±616.8 days; at the end of follow up, 6/8 discontinued PN support and 2 significantly reduced PN volume. Freedom from PN survival is 83% for the whole group; 91 and 93% for PSIL type b and c respectively, and 33% for a. Figure 1a. represents the Cox Regression for overall PN independency. The logistic regression analysis let us to build a novel formula:
Y(PN Free)= 1/(1+Exp-(5.178+3.866x[Length A=1 o Length B o C=0]+1.886x[ICV Yes=0 o No=1]+2.737x[GLP-2 Yes=0 o No=1])
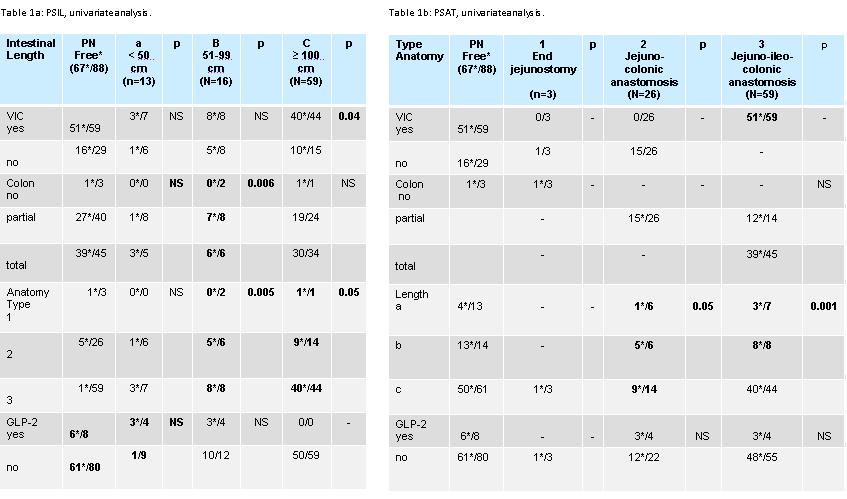
The ROC curve of the formula results for this cohort was 0.82 (Figure 1b)
Conclusions: AGIRS surgery allows converting anatomy to a favourable type for intestinal rehabilitation, as well as recovering intestinal length. TED treatment allowed later PN discontinuation in patients with unfavourable predictors. The multivariate analysis showed that PSIL, presence of ICV and the TED use, could predict freedom from PN in this cohort of adult pts
.jpg )