Introduction: Strides continue to be made in the care of patients following Intestinal Transplantation (ITx) yet, rejection continues to be a threat to its’ success. A temporary ostomy to assess the mucosa and easily perform a biopsy remains the diagnostic gold standard. However, patients with an ostomy may have high output and decreased renal function. A change in intestinal flora, as stool and mucosa are exposed to air, may trigger rejection.
Methods: We retrospectively reviewed 101 primary ITx performed from Jan 2013 to Dec 2018. 27 Isolated Intestine-Colon transplants and 7 Modified MVT were excluded. 67 patients underwent a MVT. 4 died in OR from bleeding and 1 within 72 hours thus excluded as abdominal closure was not performed. Standard immunosuppression was induction with antithymoglobulin/rituximab and maintenance with tacrolimus/mTOR inhibitor.
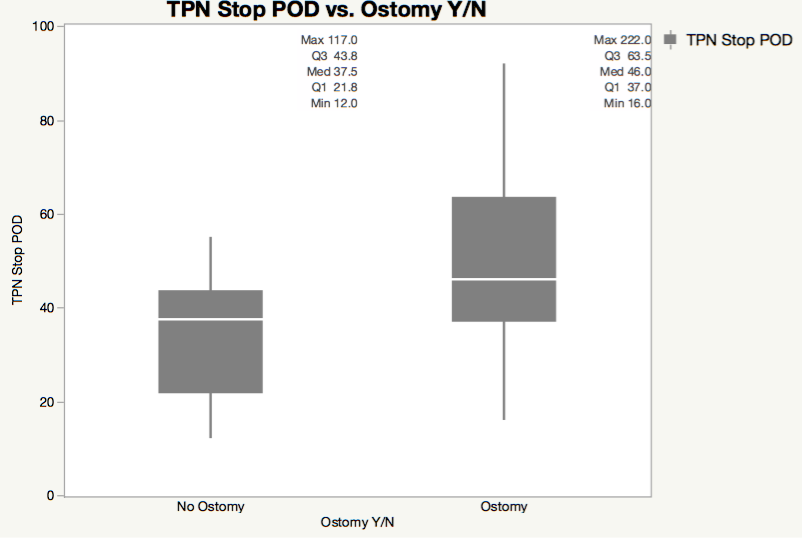
Results: Of 62 patients, 50 had 1-year follow up. 26 were pediatric (1-15yr) and 24 adult (19-68 yr). In 54% (27/50), no ostomy was performed. In 46%, an ostomy was performed- ileostomy in 12% (6/23), colostomy in 32% (16/23), hybrid colon ostomy in 2% (1/23). There was no difference between groups (Ostomy/No Ostomy) in length of stay (LOS) or admissions within the first year. LOS was 79 days with Ostomy(13-232) and 80 days (14-360) in No Ostomy. There was a trend for earlier discontinuation of parenteral nutrition in No Ostomy(32 days) vs. Ostomy(53 days).
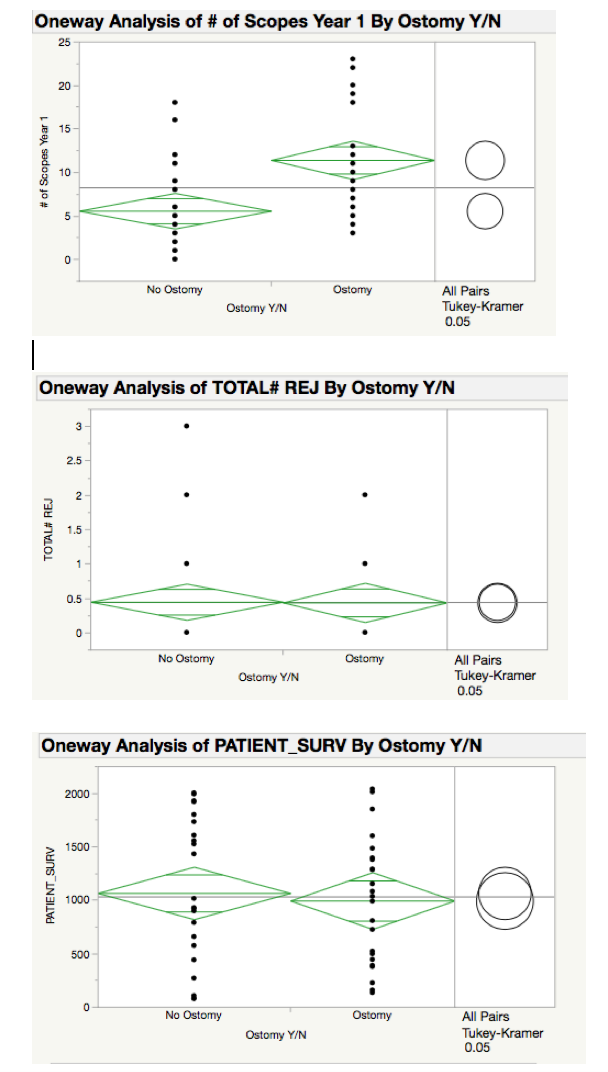
Initial endoscopy occurred earlier in Ostomy at 10 vs. 27 days in No Ostomy[F (1,48) = 15.99, p=0.0002]. Number of scopes performed in the 1st year were significantly less in patients with No Ostomy(mean = 6) vs. Ostomy(mean = 11) [F (1,48) = 15.17, p=0.0003] (Fig 2). Despite this, there was no significant difference in rejection. There was a trend toward increased rejection in patients with Ostomy(35%, 8/23) vs. No Ostomy(19%, 5/27). There was no difference in creatinine pre-transplant (non-renal) nor at 1-year post. However, the majority of patients with an ostomy (colostomy + hybrid colon) had colon in continuity making dehydration less likely. Patient 1-year survival did not differ at 82% (4/23) for those with Ostomy and 78% (6/27) with No Ostomy.
Conclusion: MVT without an ostomy continues to be feasible and safe without an increased risk of rejection nor death. Postop care seems to be easier and preservation of kidney function may impact long term ITx outcomes. Lack of ostomy greatly adds to patient satisfaction and quality of life.
.jpg )